

It was a humid afternoon in Niali—a small block in Odisha—when I first met Anita. The heat feels sticky in my memory, the kind that signals the coming of rains. This makes me think it was probably the month of June, in 2023.
Anita was around 50 years old then and a mother of two; she was battling knee osteoarthritis that had slowly chipped away at her mobility. Even crossing her own courtyard had become a struggle. Yet, despite the pain and exhaustion, she had endured an hour-and-a-half-long auto ride on rough village roads just to reach the rehabilitation camp.
I had been a physiotherapy intern back then, full of confidence in all the theory I had learned. But I hardly understood the ground reality of why tried and tested interventions failed to show results in some patients..Back then, I was almost certain that if an intervention did not work, the fault lay with the patient.
So when Anita told me that her pain hadn’t subsided even though her months-old prescription showed that she was advised to use a home-based exercise program with online video support, I instinctively believed that the shortcoming was on her part, not the treatment itself.
When I gently asked why she hadn’t been able to follow the simple home exercises we had recommended earlier, she looked at me with both fatigue and frustration. Then her words poured out in one breath:
"Dr. Babu, mera beta kehta hai video phone mein dekh lo. Lekin phone toh uske kaam ka hai, din bhar uske paas hi rehta hai. Network kabhi rehta hai, kabhi nahi. Video angrezi mein hota hai, mujhe samajhne mein mushkil hoti hai. Ghutnon ka dard rehta hai, baar-baar uthkar screen kahan dekhun? Aur jab phone bandh ho jaata hai, mera ilaaj bhi bandh ho jaata hai."
(“My son tells me to watch exercise videos on his phone. But the phone is his; he uses it all day for work. The network comes and goes. The videos are in English, and I struggle to understand. With my knee pain, how often can I keep standing and bending to look at the screen? And when the phone is switched off, my treatment is switched off too.”)
Her words stayed with me.
On paper, the idea of digital health is full of promises — physiotherapy apps like “Kaia Health” or “Sword Health” that design guided exercise programs, online platforms such as “Resolve360” that connect patients with therapists, and even AI-powered posture trainers like “Upright Go” or “Lia” exist. Alongside that are the countless YouTube tutorials that claim to make recovery easier.
But in Anita’s reality, none of these existed. They were hidden behind language barriers, unreliable internet, and the simple fact that the only smartphone in the household did not belong to her.
The Promise and the Pitfalls
As a physiotherapist and now a public health student, I have seen both sides of this story.
We often celebrate innovations in health technology - wearables that track heartbeats, apps that detect depression, and AI tools that read X-rays faster than doctors. Yet, in the communities I meet, those who need such solutions the most — people like Anita, elders with poor eyesight, families sharing one basic phone — are the very ones left behind.
I remember those days in Titlagarh, a Municipality in Balangir district of the Indian state of Odisha (it was perhaps in September of 2023), during my voluntary work with an NGO named ASSA, where I was given the responsibility of supporting the rehabilitation of children with delayed milestones.
We were trying to use the Avaz app, a picture- and text-based AAC (Augmentative and Alternative Communication) app that helps children with complex communication needs express themselves and learn how to communicate better.
But even before the therapy could begin, the first hurdle appeared—the login page was entirely in English. I watched parents struggle with something as simple as signing in, long before their children could benefit from what the app had to offer.
Another moment that has stayed with me comes from Muribahal, a small village near Titlagarh. I was there during a health camp on the birthday of Saint Bhima Bhoi, when a few villagers opened up to me in conversation.
They said they had uninstalled so-called “free” apps like Practo—not because the apps were useless, but because they ate up too much data and drained their phone batteries. In those Naxal-affected areas, where reaching a hospital or doctor is already a long and uncertain journey, the phone is often the only fragile bridge to healthcare. And yet, even that bridge felt too heavy for them to carry.
These were not small glitches. They revealed something deeper—that while innovators claim that they design new technologies to help people, it became obvious that they are trying to help a small subset of privileged people. The people these apps cater to are the urban elite, who know English, own smartphones, and are confident navigating apps.
However, these are also people who already have the safety net of living next to hospitals, private clinics, and specialist doctors when things go wrong. For them, digital health is a convenient add-on, another layer of comfort.
But for someone like Anita, who does not have those options, technology is not a luxury—it is the only possible bridge to care. And when that bridge is designed for someone else, it leaves her stranded on the other side.
Naming Exclusion
That experience also revealed what doesn’t work. Apps that shut down the moment the internet drops lose their purpose in places where the network is always patchy. Platforms that exist only in English or Hindi quietly leave out those who speak only their local tongue, making the whole system feel foreign before it even begins.
Many tools are built on the assumption that everyone has their own smartphone, when in reality, one device often has to be shared among four or five family members. And wearables, priced higher than a month’s wages for a daily laborer, are less a health solution and more an unreachable luxury.
On glossy brochures and in conference halls, these innovations sound like the future. But in villages like Niali, they are a reminder of how unevenly that future is distributed, and how easily technology can widen the gap instead of closing it.
A Different Future
That day in Niali, I found myself asking: What if health technology were designed for Anita from the very beginning?
I imagined an app with an Odia voice guiding her step by step: “Ab ghutna dheere modhiye” (“Bend your knee slowly.”)— no reading, no English, just a clear, human-sounding voice. I imagined it working offline, so she wouldn’t have to wait for network bars.
Later, I came across a pilot project in another district where community kiosks were set up at panchayat offices. People without smartphones could walk in, use a large screen to follow exercises, receive feedback, and even carry home simple pictorial instructions. At the time, it was only a pilot, but today those kiosks have been successfully installed in selected health centers in Nimapara district of Odisha. And I couldn’t help thinking if only Niali had such a kiosk back then, Anita wouldn’t have had to depend on her son’s phone.
But I also learned that solutions don’t always have to be high-tech. I began making illustrated exercise guides — bold, easy drawings Anita could pin on her wall. I filmed her once, using her son’s phone, so she could copy herself without confusion. To my surprise, she found these small steps far more useful than polished English-language videos online.
They weren’t grand innovations. They were small, thoughtful adjustments. Yet, for Anita, they made all the difference.
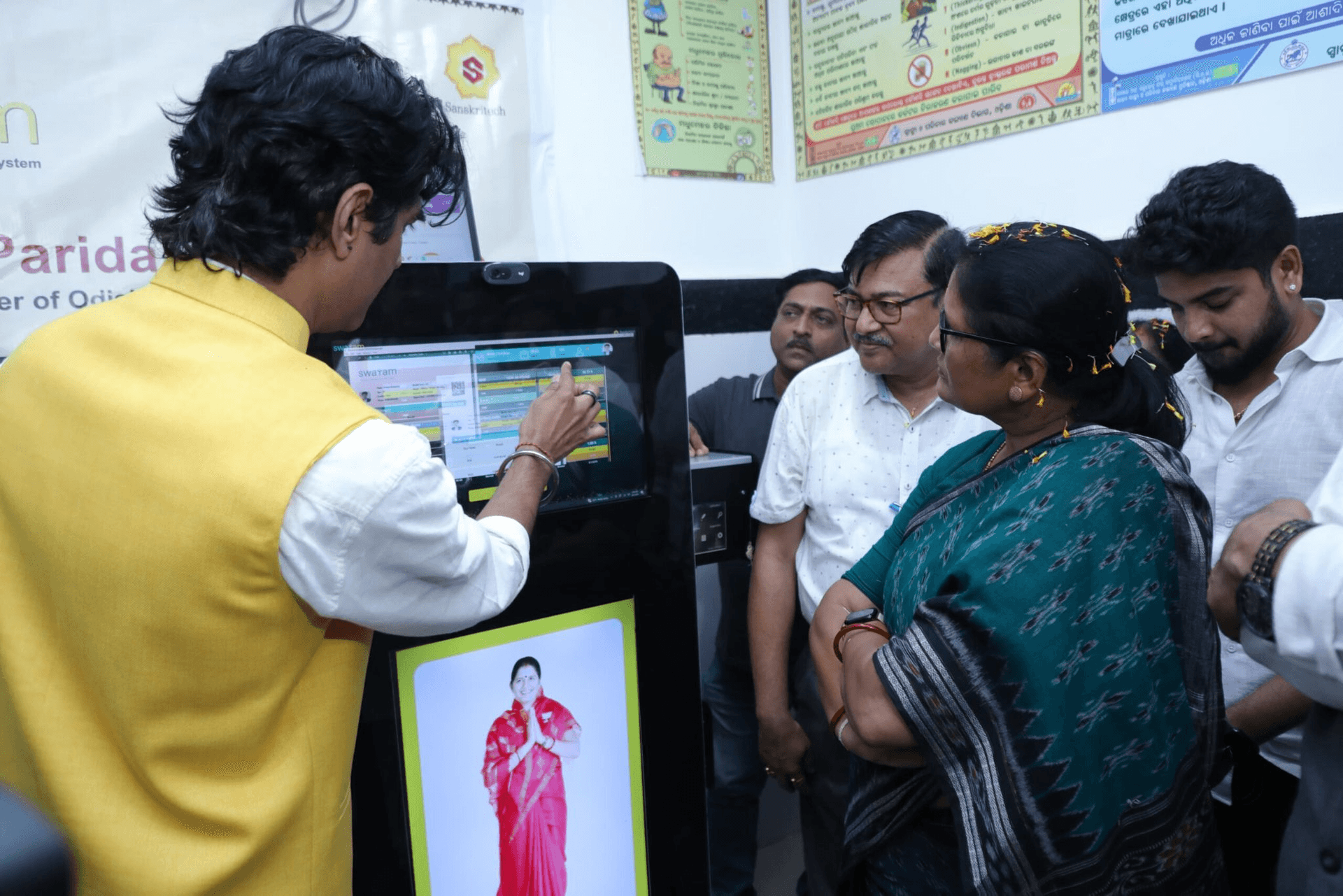
Exercise kiosk at Nimapara, Odisha. (Photo sourced from Google)
The Human Lesson
Anita taught me much more than osteoarthritis. She revealed the invisible cracks in our health system — the digital divides that stop people from healing.
When she finally practiced with the chart and her own recorded video, she smiled through her pain and said: "Ab lagta hai main apne dam pe kar paungi." (“Now I feel I can do this on my own.”)
That moment has never left me. Technology is not truly effective just because it is advanced or fashionable. It becomes meaningful only when it makes someone feel capable again, when it restores a bit of dignity, when it actually reaches the last person waiting in line.
But the reality is often harsher.
Most tech companies aren’t chasing dignity or access—they are chasing markets. Success, for them, is measured in who can pay the most and how much profit can be made.
And that leaves us with a difficult question: how do we bring these two worlds together—the need for business to sustain itself and the moral duty to care for those who cannot always pay?
There are glimmers of hope. Rwanda, for instance, uses drones to carry life-saving medicines across mountains to remote villages. In India, government-backed digital health platforms are slowly trying to make access universal. These stories remind us that technology can move beyond profit margins. What it takes is intent—the intent to place people before markets, dignity before data.
Digital health will not change lives if it stays locked inside glossy apps or English-only prompts. It will change lives when it bends down — like a physiotherapist beside a patient — to meet people where they are.
Equity cannot be an afterthought. It must be built into the design.
Because the future where digital health empowers everyone is not imaginary.
It is possible. It is urgent. And in Niali, it has already begun — with one hand-drawn chart, one borrowed phone, and one determined mother.
Edited by Christianez Ratna Kiruba
Image by Janvi Bokoliya




