
Ludhiana, Tarn Taran, and Amritsar, Punjab: At 4:40 am on May 4, 2026, a 40-year-old male patient came to Khanna Sub-divisional Hospital’s emergency department complaining of sweating and chest pain.
Within minutes, the staff nurse and Emergency Medical Officer (EMO) sprang into action-- checking his vitals, blood pressures, blood sugar, and importantly conducting an echocardiogram (ECG). The ECG result was sent on WhatsApp to the hospital’s medicine consultant, Dr Shiney Aggarwal, who diagnosed it as a ST-elevated Myocardial Infraction (STEMI) case and asked the EMO to administer the injection tenecteplase.
(Dr Shiney Aggarwal with the emergency staff at SDH Khanna)
STEMI is a severe, life-threatening heart attack with a 100% coronary artery blockage. The injection tenecteplase is used for thrombolysis or dissolving the clot, by acting on the protein holding it together, restoring blood supply to the heart.
The patient received the injection within half an hour of his ECG results and soon felt relief. Out of danger, he was kept in the hospital for observation and then referred to the Government Medical College, Patiala (54 km) for further investigations and treatment.
This case is significant because it was the 100th thrombolysis case of the hospital and the highest recorded by any centre in Punjab. A few years ago, any chest pain patient in secondary health centres like sub-divisional and district hospitals like this, would not have received treatment other than a few blood thinners and statins (cholesterol medications) and would have been asked to go to medical colleges for further treatment. The 40-70 minutes that the patient lost in transportation and further diagnosis would mean irreversible damage to his heart muscles and his ability to work in the future.
An ICMR project becomes a State-wide Mission
Since July 2025, the Punjab government has implemented Mission AMRIT (Acute Myocardial Reperfusion in Time) across the state, where staff members of sub-divisional hospitals and district hospitals (spokes) are equipped with drugs, equipment, and training to conduct thrombolysis under the guidance of a cardiologist or a specialist in the medical colleges (hubs).
Till date, about 34,000 patients with chest pain have been registered in the spokes, out of which 1900 were identified as STEMI cases, 900 have received thrombolysis, and many of them received angiography and angioplasty in the hubs. The initiative has expanded the work done by the Indian Council of Medical Research (ICMR)’s STEMI ACT project, implemented in one district of 7 states and one union territory between 2020 and 2024.
“It is very heartening to see that patients who would not have been able to afford the injection worth Rs. 30-35,000 are receiving the treatment free of cost in centres close to home within minutes-- saving their lives,” said Dr Hitinder Kaur Kler, Director Health Services, Department of Health and Family Welfare, Punjab. What’s great is that this work has been going steady even in districts that are considered challenging, like [Pakistan bordering districts] like Tarn Taran and Ferozpur, he said.
How the model works is simple--each spoke centre requires basic infrastructure like an ECG machine, a defibrillator, a heart monitor, and a fridge to store the injection. Then the staff (nurse and emergency medical officers) are trained in conducting and interpreting ECG and administering the injection tenecteplase. Medical officers and specialists in the spoke are then added to WhatsApp groups with cardiologists in the hubs who advise the course of treatment based on the ECG results of the patients.
A roster of cardiologists and MD medicine specialists is maintained in the hub to ensure support day and night. If a person with STEMI reaches the spoke within the time frame (up to 12 hours of heart attack) and has no complications, they get thrombolysed and are referred to the hubs for further angiography and angioplasty. This strategy is known as the pharmaco-invasive strategy and is ideal for low-resource settings like ours, with only a handful of catheterisation labs to conduct angiographies and angioplasties in the government sector and a large patient burden.
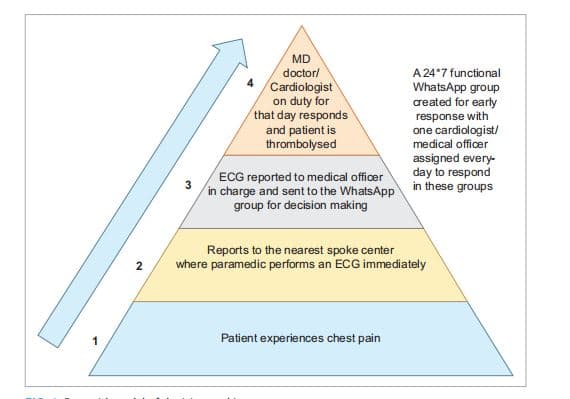
(Pyramid model for thrombolysis decision making, credit: DMC Ludhiana)
In Punjab, Ludhiana district’s Hero Dayanand Medical College’s (DMC) Chief Cardiologist, Dr Bishav Mohan, acted as a Principal Investigator for the ICMR STEMI ACT project, working with 12 spoke centres.
Initially, there was a lot of hesitancy and fear among the medical officers in the spoke centres--due to the high cost of injections, lack of confidence in reading the ECGs, and fear of the side-effects of the injection, Dr Mohan said. The medical officers, nurses, and paramedics received repeated in-person training as well as on-call and WhatsApp clinical support in reading and interpreting the ECGs. From conducting no thrombolysis in 14 cases of STEMI recorded in the system between March and July 2021, the centres conducted 238 thrombolysis in 243 eligible STEMI patients between 2021 and 2024.
While the centres upgraded and staff grew confident, patients with chest pain also started visiting the centres by word-of-mouth and awareness campaigns. From seeing only 179 chest pain patients and conducting only 50 ECGs in the baseline study, the centres after the ICMR project began, examined 3183 chest pain patients and conducted 3147 ECGs between 2021 and 2024.
While the centres upgraded and staff grew confident, patients with chest pain also started visiting the centres by word-of-mouth and awareness campaigns. From seeing only examining 179 chest pain patients and conducting only 50 ECGs during the baseline observation study, the centres after the ICMR project began, had managed to examine 3183 chest pain patients, and while managing to record ECGs, conducted 3147 ECGs of them between 2021 and 2024.
Much of this started with attitudinal shifts- secondary health care centres like district hospitals and sub-divisional hospitals, flooded with OPD patients, were not used to providing inpatient care for serious ailments, especially heart issues. “It took about two years for us to motivate the doctors and the nurses to handle emergency heart patients as they were hesitant due to the fear of managing acute emergency conditions at a secondary health care level,” said Dr Ashu Gupta, NCD cell, Department of Health and Family Welfare, who was instrumental in implementing STEMI across districts. “We are happy that despite the challenges, we are able to run the project successfully without any additional manpower,” she said.
Getting appropriate care in the spokes has also had a great effect in improving patient outcomes in the medical colleges. Amritsar's Government Medical Centre(GMC) acts as a hub for six districts around it. In the past 10 months, the hub received 272 patients who were thrombolysed in the spokes, out of which 265 underwent angioplasty at the centre.
Over the past 10 months, the project has covered 7-8 districts, with 272 patients thrombolysed and 265 undergoing angioplasty. Many of them could avail the procedure free of cost under Ayushman Bharat-Pradhan Mantri Jan Arogya Yojana (AB-PMJAY) or the Punjab government’s Mukhyamantri Sehat Bima Yojana that provides Rs. 10 lakh coverage to each family. Dr Parminder Singh Manghera, Assistant Professor, Cardiology at GMC and Nodal Officer for the STEMI project, said the mortality of the patients has dropped below 30% thanks to the model.

(Dr Parminder Singh Manghera, Assistant Professor, Cardiology, with the nursing staff at GMC Amritsar)
“Further, it has improved not only clinical outcomes but also social and economic aspects, as timely treatment prevents heart failure and loss of livelihood, especially among working-age adults,” Dr Gupta said.
Further, the hospitals in the spokes continued providing thrombolysis in the border areas in challenging circumstances like during Operation Sindoor and devastating floods in August 2025--worst in four decades--affecting 13 out of 23 districts, he added.

(Dr Bishav Mohan, pointing to the ECG recieved on the Mission AMRIT Whatsapp group)
Running the programme across the state
The success of the project is thanks to the tireless efforts of health officials like Dr Gupta, who spends a lot of her personal hours engaging with doctors in the centres through WhatsApp groups, coordinating with them, collecting data, and also maintaining the supply of tenecteplase across 65 centres in the state. Similarly, Dr Bishav Mohan spends many of his hours every day answering queries, advising the doctors on the treatment required, and encouraging them to conduct more thrombolyses through multiple WhatsApp groups.
The emergency department of any district or sub-divisional hospital is a place of constant chaos. There are 1-2 Emergency Medical Officers and a staff nurse dealing with everything from obstetrics cases, accidents, pediatric cases, and dealing with medical legal cases. Medical Officers deal with 100-200 patients in their OPDs with many administrative tasks and additional duties during melas, pilgrimages, and elections, while facing frequent transfers.
Add to this infrastructural gaps, staff shortage, and patient numbers; keeping these overwhelmed medical teams interested required motivational talks, treating nurses as equal partners, use of Punjabi languages during training and technical materials, and awarding best performers from the districts on a monthly basis, and also organising an award ceremony by the health minister, said Dr Mohan. “Once people start working, they see that they are able to save lives; this in itself is a morale booster and keeps them performing,” he said.
Involvement of Private Centres
A unique feature of ICMR’s project in Ludhiana was that it was led by Dr Bishav Mohan, who works in a private medical college and who continues to provide the technical support in Mission AMRIT. “I was one of the volunteers during the COVID pandemic and also worked together with the government as a Convenor of the COVID group,” he said.
This and the fact that he studied in the All India Institute of Medical Sciences, Delhi, helped him gain ICMR and the state government’s confidence. “There was no red tape from either the (DMC’s) management or the government side,” he said. This also helped Dr Mohan’s team to arrange gap funding to secure or repair certain equipment, like ECG machines or defibrillators, in centres that did not have them through philanthropy. Another exception of the Ludhiana project was the inclusion of three private centres as spokes in the pilot.
One of them was Lifecare Hospital, a small 20-bedded private facility, catering to a mostly rural population 38 km from Ludhiana in Raikot. “We used to use streptokinase injection for thrombolysis before, but there was a risk for anaphylaxis [fatal allergic reaction], and it took 45 minutes to administer. With this project and tenecteplase, we got excellent results,” said Dr Simarjit Singh Sindhu, MD, Medicine, and co-owner of the hospital. The hospital conducted 52 thrombolyses in two years, and the door-to-needle time was just 8 minutes, he said. “Our staff was trained, and patients were really happy in getting the injection free of cost, as most of them don’t have the paying capacity,” he said.
However, since the ICMR project ended in 2024 and private centres are not part of Mission AMRIT, the centre cannot treat patients free of cost as before. “The numbers have dropped; now we get one patient every three months,” he said.
STEMI models pan India
After the successful Tamil Nadu-STEMI pilot that showed how a hub and spoke model can improve reperfusion rates and reduce mortality, this model was implemented in many states, including Tamil Nadu, Goa, Karnataka, Andhra Pradesh, etc. In most states, spokes are Community Health Centres (CHCs), sub-divisional hospitals, and district hospitals, and with medical colleges with cath labs being the hubs.
“In our study, at least around 8000 patients have been thrombolised, and we are able to almost triple the thrombolysis rate where nothing was happening before,” said Dr S Ramakrishnan, consultant cardiologist at AIIMS and National Principal Investigator, ICMR ACT project that concluded in December 2024. He said the current focus of the study is on increasing access to thrombolysis and not increasing the rate of angioplasties due to paucity of cath labs and the high cost of the procedure.
Tamil Nadu has been the most successful state, which has thrombolysed over 72,000 patients over five years, with 67% annual increase in STEMI patients receiving thrombolysis and 68% increase in patients receiving primary angioplasties.
But including only the government hospitals as hubs is reducing the effectiveness of the model, said Dr Thomas Alexander, who, along with Dr Ajit Mullasari, piloted the TN-STEMI model. “Out of 350 cath labs in Tamil Nadu, only 20 are in the government set-up, which is why only 20% of STEMI patients currently receive reperfusion in the government sector,” he said.
Given that reperfusion should occur in the first 3–4 hours for reducing long-term morbidity and mortality, integrating both public and private reperfusion centres into a unified STEMI network, supported by independent audit and quality improvement systems, would improve timely access and outcomes, he said. “Patients covered under government insurance schemes should have access to the nearest reperfusion centre—public or private—with safeguards to prevent overuse and overcharging,” he said.
Dr P C Negi, who headed the cardiology department of Indira Gandhi Medical College, Shimla, and acted as Principal Investigator of the Shimla centre of the ICMR ACT project, agrees.
“In the state of Himachal Pradesh, there are only 7-8 centres with Cath labs,” so the model should include all centres with cath lab facilities in the state so that the patients have a choice where to receive the treatment and all patient data is captured in the system,” he said. In Himachal Pradesh, the STEMI hub-and-spoke model is implemented statewide but lacks comprehensive data capture, needs more community awareness, and PHC inclusion to reduce treatment delays and improve outcomes, he added.
The Way Ahead
In Punjab, a year after Mission AMRIT’s implementation, some limitations of the model are obvious--it relies on individual interest and effort. While some spokes like SDH Khanna are doing exceptional work, many other spokes have only conducted a handful of thrombolyses despite the availability of drugs and trained staff. Also, at the moment, there is no follow-up as to what happens to patients after they leave the hubs. This follow-up with tertiary care institutes is part of the next phase of the mission, said Dr Mohan.
There are many bright spots, though. The momentum of the STEMI project has encouraged the state officials to use district hospitals and sub-divisional hospitals for emergency treatment of stroke patients in a similar hub and spoke model, as the same drug tenecteplase is used for both.
For both STEMI and stroke, what is important is that patient reaches the medical facility in the golden hour, thanks to the project there is more awareness in people and they are turning up early, “We are seeing more women from villages above the age of 50 with symptoms turning up in spoke centres because it is close to home and accessible, we would have missed this demographic before,” said Dr Mohan.
Edited by Christianez Ratna Kiruba
Image by Swagata Yadavar
This story is the second part of a three-part series on cardiac care supported by Sunfox Tecchnologies
It was published initially in The Hindu on this link




